
Priority 4b Action mortality, morbidity and experience
Maternal Medicine Networks (MMN) are central to NHS England’s Improvement strategy for reducing mortality for all pregnant woman and reducing neonatal morbidity and mortality. The aim of MMNs is to ensure women with acute and chronic medical problems have timely access to specialist advice and care at all stages of pregnancy. The need for MMN has never been greater. The 2024 MBRRACE report highlighted an increasing maternal mortality rate in the UK as well as persistent inequalities in experiences and outcomes of maternity care across the country. MMNs are an essential element of improving safety and reducing inequalities. The 2022 Ockenden review acknowledged the progress made around the creation of maternal medicine networks nationally and recognised their important role in enhancing the care and safety of complex pregnancies. This was reiterated in the 3 Year Delivery Plan for Maternity and Neonatal Services, which is clear that every woman in England should be able to access a nationally networked and collaborative MMN.
MMN’s bring together multidisciplinary teams of obstetricians, physicians, midwives, and other specialists to provide comprehensive, coordinated care for women with pre-existing health issues or those who develop medical complications during pregnancy. The networks play a critical role in improving equity of care by standardizing best practices and ensuring that pregnant women, regardless of location, have access to the same level of expert treatment. This collaborative model helps prevent maternal morbidity and mortality, while also improving patient experience through better continuity of care.
Key drivers for creation of maternal medicine networks nationally
- Rising Maternal Morbidity and Mortality
- Reports from MBRRACE-UK (Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries) highlighted that maternal deaths from indirect causes (e.g. cardiac, neurological disease, sepsis) now exceed those from direct obstetric causes.
- Over two-thirds of maternal deaths involved women with pre-existing physical or mental health conditions.
- Need for Specialist Multidisciplinary Care
- Pregnancy significantly alters physiology, requiring specialist input from physicians with expertise in managing medical conditions during pregnancy.
- Many conditions are rare, so centralising care in designated centres improves outcomes by concentrating expertise.
- Health Inequalities
- Women from Black, Asian, and minority ethnic backgrounds, and those from socially deprived areas, are disproportionately affected by poor maternal outcomes.
- MMNs aim to tackle these disparities through focused, inclusive, and accessible care.
- COVID-19 Pandemic Lessons
- The pandemic exposed vulnerabilities in maternal care systems, especially for women with underlying health conditions, reinforcing the need for robust, networked services.
Policy directives and frameworks
- NHS England Maternal Medicine Service Specification (2021)
- Official guidance published in October 2021 outlines the scope, structure, and expectations for MMNs.
- It mandates care across the pre-pregnancy, antenatal, and postnatal periods for women with significant medical conditions.
- NHS Long Term Plan
- Emphasises improving maternity safety and outcomes, particularly for women with complex needs.
- Three-Year Delivery Plan for Maternity and Neonatal Services (2023)
- Sets out goals for equity of access, multidisciplinary collaboration, and data-driven evaluation of maternal services.
- Women’s Health Strategy for England (2022)
- Recognises maternal health as a priority area and supports integrated, personalised care models like MMNs.
Network footprint and services
Maternal Medicine services within the North West are provided within three localities Lancashire and South Cumbria, Cheshire and Merseyside an Greater Manchester which together form the North West Maternal Medicine Network (NW MMN). In order to maintain the ethos of care closer to home, the NW MMN is split in to three localities each offering a designated Maternal Medicine Centre (MMC); St Marys Hospital- Manchester University NHS Foundation trust, Liverpool Women’s Hospital and Royal Preston Hospital- Lancashire Teaching Hospitals NHS Foundation Trust. In addition there are 18 maternity providers delivering care across the three localities. Figure 1 below outlines the geographical spread of maternity provision across the networks footprint and identifies the 3 MMCs.
The MMN networks all maternity providers through the MMCs by further developing existing care pathways and creating new pathways and clinical guidelines as service provision and expertise develops. Every Trust within the region that provides maternity services (any level) is a member of the NW MMN. All constituent providers within the network will be responsible for agreeing and upholding shared protocols on the management and referral of women with medical conditions. This model of care will ensure that – where agreed appropriate – investigation and management is carried out by an experienced Multidisciplinary Team (MDT). The majority of women with complications during pregnancy will continue to be managed by their local maternity service. The proportion of care delivered by a MMC will vary according to individual need. For some, a single visit to the MMC or communication with the MMC by the local unit will suffice. For the most complex cases, it may be recommended that all care is delivered within the MMC.
Lancashire and South Cumbria Maternal Medicine Centre Composition- Lancashire Teaching Hospital
- Three maternal medicine consultants
- No obstetric physician
- 1 network funded specialist midwife
- 1 network funded MDT coordinator
- Receive approximately 50 referrals a month
- Establishing joint specialist clinics and these are supported by specialist obstetric physicians
Local population data
Double the number of females of reproductive age living in decile 1 – 22.3% compared to England average of 11.1%
- Nearly 1/5 live in a rural area with associated challenges
- Many of L&SC districts fall within the worst quintile for female inequality in life expectancy at birth year after year
NW MMN objectives
- Facilitating telemedicine to enable networked involvement in the multi-disciplinary team
- Life course care provision developing pre-conception/ postnatal care standards of practice
- Developing clinical models of care to support providers and standardise care
- Retrospective review of Northwest maternal deaths- region wide action plan to address recommendations and areas of learning
- Developing a research strategy
- Supporting Local Maternity and Neonatal System (LMNS) assurance visits and attending LMNS boards and working groups.
- Understand what the additional funding requiremants are to develop the NW provision and enhance MMCs-support business case proposals
- Develop a national profile to inform policy developments and share experiences, learning and progress with other regions.
- Developed an accredited maternal medicine master module, now commenced at the University of Bolton
- Facilitated maternal medicine training events/ study days
- Supporting the Obstetric Medicine RCP training centre
- Professional Aftercare Toolkit (PACT) is under development to support midwives who experience traumatic events during their practice.
- Redesigning and refocusing networks engagement and co-production strategy.
- Developed website as a resource to direct patients to support and information
- Platform for referrals established and regional referral pathway implemented
- Regional guidelines developed around diabetes and cardiolgy and further guidelines are under development
- Regional Maternal Medicine Midwifery and Specialist Nurse forum.
Offer referral to the NHS Diabetes Prevention Programme to women with a past diagnosis of Gestational Diabetes Mellitus (GDM) who are not currently pregnant and do not have diabetes once a blood test has identified that they no longer have diabetes at 6-12 weeks.
Gestational diabetes, as defined by the NHS, is high blood sugar during pregnancy that typically resolves after birth. It’s usually diagnosed in the second or third trimester and symptoms include increased thirst, frequent urination, fatigue, dry mouth, vision problems, and itchiness or thrush.
Women are at increased risk of developing gestational diabetes if they:
- Are over 40 years old
- Have a BMI above 30
- Have previously had a baby who weighed 4.5kg or over at birth
- Have previously had gestational diabetes
- Have a parent or sibling who has diabetes
- Of south Asian, Black, African-Caribbean or Middle Eastern origin (even if born in the UK)
- Have had weight loss surgery

The local provider of the diabetes prevention is Healthier You | Diabetes Prevention
Insights that inform the drive
Women who have had gestational diabetes are at higher risk of developing type 2 diabetes later in life and of developing gestational diabetes in subsequent pregnancies in fact “up to 50% of women diagnosed with gestational diabetes develop type 2 diabetes within 5 years of the birth” Healthier You | Diabetes Prevention.
Download the physical-activity-gestational-diabetes.pdf advice leaflet on gestational diabetes from healthier you.
Infographic below:

This infographic shows the recommended amount of exercise recommended during pregnancy which is 150 minutes of moderate activity per week. It explains the benefits of this, improved sleep and mood, decreased risk of developing gestational diabetes, reduced risk of high blood pressure and weight gain and improves fitness.
This infographic shows the amount of recommended exercise after birth which if 150 minutes of moderate intensity activity a week in the first 12 months. Lists the benefits of this. Encourages the individual to build up exercises gradually.
Get active – Better Health – NHS
Why is it important?
Type 2 diabetes is a long-term condition which can detrimentally affect an individual’s quality of life. It causes high blood sugar levels either due to the body not producing enough insulin or the insulin that the body makes not working properly (which is known as insulin resistance) (Diabetes UK). People living with type 2 diabetes have a higher likelihood of developing conditions such as heart attack, stroke, problems with eyes and feet alongside other complications. Many individuals do not experience symptoms or feel unwell so it can go undetected. When women have experienced gestational diabetes, they are more likely to go on to develop type 2 diabetes and should therefore have annual blood tests, so this does not go undiagnosed.
Certain risk factors for type 2 diabetes, like ethnicity or medical history, cannot be changed. Modifiable factors include eating well, maintaining a healthy weight and waist size, and increasing physical activity. Women at higher risk should have access to prevention programmes.
“Research has shown that for some people a combination of lifestyle changes can reduce their risk of type 2 diabetes by about 50%” (Diabetes UK)
The plan (Equity plan)
What have we already achieved?
A working group has been established with the prevention team from the ICB and the diabetes lead midwife from each trust. Looking to standardise practice across the LMNS by using an automated digital system to send letters to GP surgeries advising about the 6-12 week postpartum diabetes screening, blood test, and onward referral to prevention services.
What are we working on?
Enhanced continuity of carer teams are being introduced across LMNS to ensure women receive consistent care from the same midwife team before and after birth. This approach leads to improved outcomes for mothers and babies and supports better information sharing and management of gestational diabetes.
The working group is collecting data to analyse the uptake of the prevention programme. Looking at ways to improve uptake of this. Diabetes midwives are meeting with Reed the prevention provider to understand better the structure and content of the prevention course so that they are more informed when discussing this with their clients. The working group is also looking at other ways to make referrals to improve uptake of the prevention programme. Through this REED have now been linked with the 0-19 service and are attending workforce training to make health visiting services more aware of the prevention programme.
Each of our four NHS Trusts has a lead diabetes midwife.
Training for staff
CPD modules from Diabetes UK Home | Diabetes UK CPD
Resources
Care Pathways
The Lancashire and South Cumbria LMNS has prioritised antenatal care for women with complex social factors through its Equity & Equality programme, embedding this group as a specific system‑level intervention. Support has been strengthened through flexible service specifications, delivery of antenatal care via family hubs and community settings, co‑production with women least likely to engage with traditional services, integration with personalised care and support planning, and partnership working with voluntary and community organisations. This approach recognises and addresses barriers such as deprivation, language, digital exclusion and social complexity to improve access, experience and outcomes.
1. Explicit system priority within the LMNS Equity and Equality programme
- Antenatal care for women with complex social factors is identified as a specific intervention within the LMNS Equity & Equality programme under Priority 4b: Action on mortality, morbidity and experience.
- This places complex social factors alongside other high‑risk equity priorities and ensures system‑level oversight rather than isolated local initiatives.
2. Embedding support for complex social factors in maternity service specifications
- The Lancashire & South Cumbria Maternity Service Specification (FY 2025/26) sets system‑wide expectations that allow providers to tailor antenatal care for women with additional social vulnerability, including:
- flexible, locality‑based delivery models
- escalation and safeguarding processes aligned to regional policy
- The specification enables differentiated models of antenatal care to meet the needs of women with complex social factors, rather than a one‑size‑fits‑all approach.
3. Use of Family Hubs and community‑based antenatal provision
- The LMNS has supported the delivery of antenatal care through Family Hubs and community venues, reducing reliance on hospital‑based appointments alone.
- Family hubs provide:
- accessible, local settings
- face‑to‑face, virtual and outreach options
- opportunities for integrated support with wider health, wellbeing and social services
- This model is particularly beneficial for women experiencing deprivation, instability, or barriers to accessing traditional maternity services.
4. Co‑production with women least likely to engage with antenatal services
- The LMNS has undertaken targeted antenatal co‑production activity focused on women who typically experience barriers to engagement, including:
- women living in the most deprived areas (IMD 1–4)
- teenage parents
- women with English as an additional language
- asylum seekers and migrant women
- women who are less likely to attend standard antenatal education
- This work identified practical barriers such as language, terminology, fear of judgement, lack of awareness of services, and limited access to interpreters, and is being used to inform redesign of antenatal approaches.
5. Linking antenatal care with personalised care and continuity
- Women with complex social factors are supported through the LMNS‑mandated Personalised Care and Support Plan (PCSP) approach, ensuring antenatal care is shaped by:
- individual needs
- social context
- wider determinants of health
- PCSPs are used as a mechanism to improve engagement, continuity and coordination of care across maternity and community services, particularly for vulnerable women.
6. Integration with voluntary, community and faith sector organisations
- The LMNS has actively engaged with VCFSE partners, including family hubs, infant‑feeding networks, food banks and community organisations, to:
- improve antenatal support pathways
- address wider social needs such as food insecurity and social isolation
- support women who may not otherwise engage with statutory maternity services
- This community‑linked approach strengthens antenatal care for women with complex social factors by addressing practical and social barriers alongside clinical care.
7. Recognition of access and communication barriers
- LMNS workstreams have explicitly recognised that women with complex social factors may face barriers related to:
- language and health literacy
- digital exclusion
- lack of trust or fear of judgement
- Antenatal support is therefore being shaped to:
- use accessible language
- offer non‑digital and face‑to‑face routes
- reduce stigma and improve engagement
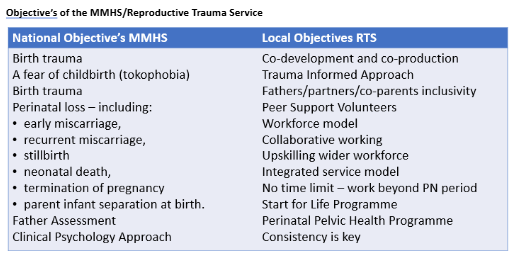
Maternal mental health services
- Reproductive trauma service
Long Term Plan Ambitions

Ambition 1 – To offer access to specialist assessment & evidence based treatment with a focus on psychological interventions in line with NICE guidance to women having moderate to severe or complex mental health difficulties with a significant association with trauma or loss in the maternity/perinatal/neonatal context and falling through the gaps of existing service provision
- Triaging cases
- Conducting initial assessments of biopsychosocial needs
- Providing advice/support and signposting to the most suitable servicesavailable
- Providing evidence-based psychological interventions
Ambition 2 – To implement an holistic, personalised and trauma informedapproach to care – within and outside of the service
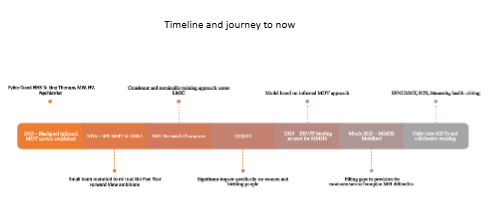
Our journey so far
- Integration of Maternity and Mental Health
- Establishing a service across the system
- Building strong foundations
- Staffing model
- Consultation and co-production
- Amending and reviewing our criteria
- Capacity and Demand
- Awards and Achievements
RTS – Eligibility criteria
The service is available to women over 16 years of age who live in Lancashire and South Cumbria
- Moderate- severe trauma symptoms directly related to a reproductive experience
- Acceptance into service based on severity of mental health presentation and impact on functioning, NOT severity of traumatic experience
- Severity of symptoms dictated by frequency, level of distress, and their impact on daily/ normal functioning
Exclusion
- Referrals will not be accepted until at least 4 weeks after the traumatic event has occurred
- Referrals will not be accepted where there is already an appropriate service available to the woman/ she is accessing appropriate support elsewhere
- Psychological therapy will not be offered for treatment of tokophobia for referrals received after 28 weeks’ gestation

A Black Cloud (experiences of birth trauma and loss) – subtitled – YouTube
Common challenges
Low access for Black Asian and Minority Ethnic people
- Increased risks for loss and poor outcomes for births 5 x more.
- Cultural and Language Barriers
- Need for tailored approaches and community engagement
- Asking for help – early intervention vs crisis
Young parents
- How do young people ask for help?
- Are we where we need to be?
- Consistency in relationships– are they in place?
- Mental health – what is their ‘norm’?
- Do we offer a more tailored approach?
Areas of high deprivation
- Travel costs to come to appointments
- Digital Poverty
- Do we tailor appointments to address need?
Feedback


Intervention 5 Personalised care and support plans
Through the Lancashire & South Cumbria LMNS, personalised care and support plans are a mandated element of maternity care, with all women and birthing people expected to have a jointly owned plan by 20 weeks’ gestation. PCSP delivery is embedded within service specifications, aligned to national personalised care policy, and explicitly linked to the LMNS Equity & Equality programme. The system has taken steps to mitigate digital exclusion by requiring PCSPs to be available in multiple languages and formats, including hard copy, and by using digital systems such as BadgerNet to support—rather than replace—personalised conversations and continuity of care across pregnancy and the postnatal period.
What Lancashire and South Cumbria LMNS has delivered on maternity personalised care and support plans
1. System‑wide requirement for personalised care and support plans
- The LMNS has embedded PCSPs as a core contractual and service requirement across all maternity providers through the Lancashire and South Cumbria Maternity Service Specification (FY 2025/26).
- Providers are required to develop a jointly owned personalised care and support plan with all women and birthing people by 20 weeks’ gestation, based on proactive conversations about:
- what matters to the woman
- her needs
- wider health and wellbeing
2. Alignment with national personalised care policy
- LMNS commissioning requirements explicitly align with:
- NHS England personalised care ambitions
- the NHS Standard Contract
- the Equity and Equality Guidance for Maternity and Neonatal Services
- The ICB role is clearly articulated as “commissioning for and monitoring the implementation of personalised care for every woman”, including oversight of PCSP delivery across the system.
3. Equity‑led approach to personalised care
- The LMNS Equity & Equality programme explicitly links PCSP delivery to reducing inequalities in access, experience and outcomes, particularly for:
- women from Black, Asian and Mixed ethnic groups
- women living in the most deprived areas
- PCSPs are positioned as a mechanism to:
- support informed decision‑making
- tailor care to individual needs
- improve experience across pregnancy, birth and postnatal care
4. Addressing digital exclusion in PCSP delivery
- The LMNS has recognised digital exclusion as a specific risk within personalised care delivery.
- Explicit expectations are set that PCSPs must be available in a range of languages and formats, including:
- hard‑copy plans for women experiencing digital exclusion
- formats compliant with the Accessible Information Standard
- This ensures that access to personalised care is not dependent on digital tools alone.
5. Use of digital systems to support (not replace) personalised care
- The LMNS has supported the use of BadgerNet and BadgerNotes as digital tools to record and share maternity care plans where appropriate.
- System‑level review work was undertaken in response to concerns that some women could not access information in a meaningful way, reinforcing the need for flexibility and alternative formats in PCSP delivery.
6. Extending personalised care into the postnatal period
- LMNS discussions and workstreams (e.g. Maternal Mortality Working Group) highlight the importance of:
- women leaving hospital with a personalised plan
- PCSPs following the woman into community and primary care
- This reflects a system ambition to strengthen continuity and postnatal experience, in line with national learning and CQC findings.
7. Monitoring and assurance of personalised care
- The LMNS has committed to:
- monitoring delivery of personalised care through audits
- seeking feedback from women and families
- acting on findings to improve equity and experience
Assurance is provided through LMNS governance structures, including quality and equity oversight arrangements.
MNVP diversity
Ensure your MNVPs in your LMS reflect the ethnic diversity of the local population in line with NICE QS167 (Statement 1 and 2)
Statement 1: Black, Asian, and other minority ethnic groups help set priorities and design local health and well being programs. Quality statement 1
Statement 2: Black, Asian, and other minority ethnic groups are included in peer and lay roles in these programmes. Quality statement 2
In 2023-24, Lancashire and South Cumbria LMNS began discussions with HealthWatch Lancashire to have them host and support MNVP Leads as a commissioned service for the LSC Integrated Care Board. This approach aims to:
- Maintain MNVP independence from the ICB or NHS Provider Trusts
- Provide admin support for MNVP Leads
- Improve data capture and reporting to the ICB
- Secure adequate budget and facilitate payments, IT, and hosting arrangements
- Promote collaborative working where relevant
- Ensure consistency across the system
- Offer MNVPs access to HealthWatch resources and support
- Ensure compliance with MNVP Guidance
In 2024-25, we began our first full year commissioning HealthWatch Lancashire, establishing a mandate for service provision. As an ICB, we also aligned our Public Sector Equity Duty with the Equity and Equality guidance related to MNVPs, with a focus on reaching seldom heard voices and empowering those voices to drive change for individuals experiencing the poorest outcomes.
Together, the LMNS, HealthWatch, and MNVPs developed a data capture system designed to record ethnic backgrounds, deprivation deciles (using postcodes), and other protected characteristics. This allows us to assess our system’s reach and identify challenges and gaps.
Engagement with minorities and seldom heard groups has grown steadily across all areas. MNVPs note the BAME label may not accurately reflect current minority groups, given the rise in refugees and Eastern Europeans. Efforts to connect with these communities have improved ties with other organizations. However, reaching Gypsy, Roma, and Travelling communities remains challenging and will be a focus for next year.
Whilst the number of unknown demographics is still relatively high, it is encouraging to note that of those recorded demographics, 46% of all service users engaged with are from the lowest quintile of deprivation, demonstrating that the MNVPs are gaining access and engagement from those seldom heard groups. Measures ae currently being implemented by Healthwatch, as detailed below, to try and reduce the number of unknown demographics and capture a more accurate picture in the upcoming year.
Key achievements
Bay Wide MNVP
- Engaged with bereaved families to incorporate their perspectives into the planning and development of a new bereavement suite at RLI.
- Established a working group of service users to undertake a sustained initiative focused on the Induction of Labour.
- Implemented a successful 360-degree feedback process involving service users, MNVP, and Trust stakeholders.
East Lancs MNVP
- The introduction of the Engagement Lead position has facilitated increased engagement with hard-to-reach groups.
- A dedicated working group was established to improve translation services and enhance communication between the Trust and service users.
- Ongoing engagement with service users, including the collection of feedback regarding issues experienced with Badger Notes.
BFW MNVP
- Volunteers have been integrated within the MNVP to support the expansion of engagement activities.
- Quarterly engagement sessions are now held at the Metropole Hotel to reach asylum seekers.
- Co-production efforts with Blackpool Family Hub and the parent panel aim to improve community access to support services.
PCSR MNVP
- Targeted engagement with individuals from minority ethnic backgrounds who have experienced PPH supports ongoing collaboration with the Race & Health Observatory.
- Engagement initiatives related to infant feeding contribute to the development of trust information and support videos.
- Feedback obtained from engagement activities has been delivered regarding the use of donor milk within ethnic minority groups.