
Priority 4c Action on perinatal mortality and morbidity
Continuity of carer in the context of NHS maternity services refers to a model of care where a pregnant woman receives support from the same midwife, or a small team of midwives, throughout her maternity journey — including antenatal, intrapartum (labour and birth), and postnatal care.
Key Features:
- Relationship-based care: The woman builds a trusting relationship with a known midwife or small team, improving communication and personalisation of care.
- Consistency: Care is coordinated and consistent, reducing fragmentation and improving safety.
- Improved outcomes: Evidence shows this model leads to better clinical outcomes for mothers and babies, and a more positive experience overall.
NHS England’s definition:
“Continuity of carer is a way of delivering maternity care so that women receive dedicated support from the same midwifery team throughout their pregnancy. This relationship… has been proven to lead to better outcomes and safety for the woman and baby.” [england.nhs.uk]
Royal College of Midwives (RCM) definition:
“Midwifery continuity of carer (MCoC) is a model that enables a pregnant woman to build a relationship with a midwife (and a small team) who provides the majority of her care across the whole continuum: antenatal, intrapartum and postnatal.”
Midwifery Continuity of Carer:
- Ensures consistent carer involvement, beginning from the identification of the care pathway at booking, and extending through the antenatal, intrapartum, and postnatal periods.
- Aims to provide continuity for 75% of women from Black, Asian, and Minority Ethnic (BAME) backgrounds and those in the most deprived groups, with specific focus on decile 1.
- This approach should prioritize geographical regions rather than focusing on individual vulnerabilities or complexities, whether medical or social.
Enhanced Midwifery Continuity of Carer:
- Involves expanding team capacity through the inclusion of an MSW/Advocate at Band 4, who facilitates support for women residing in areas of highest deprivation (IMD1).
- Objectives include enhancing peer support among women at similar stages of pregnancy, supporting access to services that address broader determinants of health, increasing women’s agency in optimizing their health, providing assistance with behavioural activation, and enabling midwives to dedicate more time directly to patient care.
Enhanced Continuity of Carer (EMCoC)
Summary of our work
- Piloted EMCoC teams across Lancashire & South Cumbria with targeted funding agreements.
- Focused on workforce modelling, start-up costs, and phased rollout to priority groups.
- Evaluation shows improved relational care and midwife satisfaction, but sustainability remains challenging.
National drivers
- Better Births Review: Advocates safer, personalised care through continuity models.
- NHS Long Term Plan: Ambition for Continuity of Carer to become the default model.
- Equity Focus: Prioritisation for women at higher risk of poor outcomes.
- Governance: Quarterly reporting and assurance frameworks mandated nationally.
National barriers
- Workforce shortages and high service demand.
- Cultural resistance to new working patterns.
- Operational pressures limiting transformation capacity.
Local barriers
- Recruitment and retention challenges for EMCoC teams.
- Infrastructure gaps (SOPs, readiness frameworks).
- Financial constraints and reliance on short-term funding.
Recommended next steps
- Strengthen workforce planning and retention strategies.
- Develop robust SOPs and readiness frameworks across all trusts.
- Secure sustainable funding for continuity models.
- Strengthen team engagement and change management support.
The gold standard remains as previously defined; teams will be implemented accordingly, depending on safe staffing.
Starting August 2025, Trusts may report compliance if they deliver continuity of care with a B4 role to boost capacity, even if:
- Continuity covers only antenatal and postnatal periods, not intrapartum.
- Continuity is provided to targeted groups (e.g., socially or medically vulnerable), rather than by geographic area.
East Lancashire Willow Team: Enhancing maternity care for Blackburn families (East Lancashire Hospitals NHS Trust)
Smokefree pregnancy
Directive/drivers
The NHS England Equity and Equality Guidance for local maternity systems action 4c intervention 2 stipulates the implementation of a smoke free pathway for mothers and their partners.
The NHS Long Term Plan has addressing health inequalities at its core and smokefree pregnancy is a priority in the Maternity Transformation Programme tobacco-control-delivery-plan-2017-to-2022.pdf (publishing.service.gov.uk) .
Although overall smoking rates have declined in the UK, this decrease has not been seen across all groups:
“As smoking prevalence has declined, it has become increasingly concentrated among more disadvantaged communities and groups” Health matters: stopping smoking – what works? – GOV.UK (www.gov.uk). Adding to health inequalities and widening the health gap between those living in different demographics. To achieve health equity and equality health services need to address this.
LSC have developed the Tobacco Strategy 2023-2028 which identifies the key objectives within the following documents:
- Saving Babies Lives Version 3
- Core20Plus5 – Maternity
- NHS Long Term Plan
- 3 year Maternity and Neonatal Delivery Plan
Insights that inform the drive
The harmful effects of smoking on health are well documented:
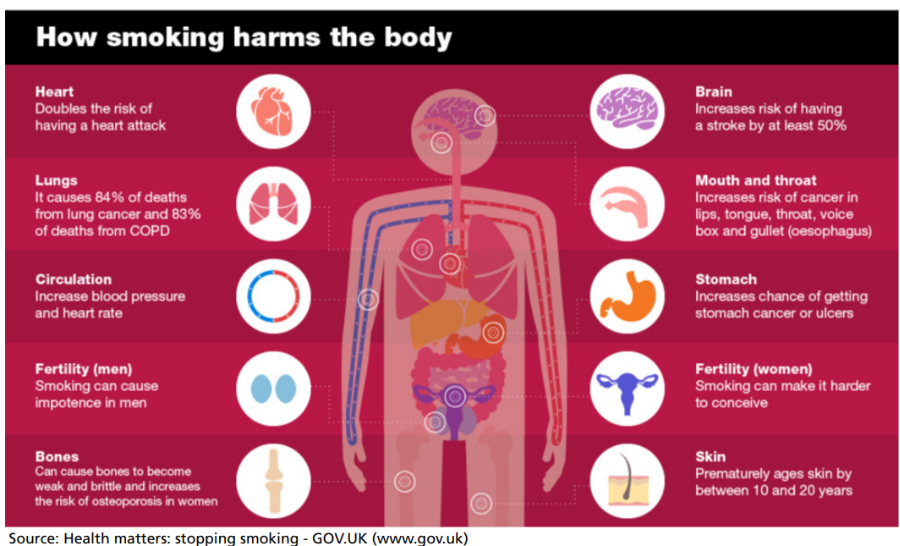
This infographic shows how each organ in a human body is affected by smoking.
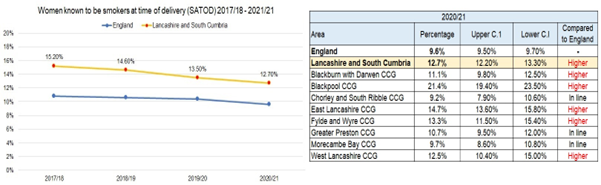
The stark figures from 2020-21 show that Lancashire and South Cumbria (LSC) perform worse than the national average of smoking at time of delivery; particularly Blackpool at 21.4% and East Lancashire at 14.7%
Why is it important?
Stopping smoking during pregnancy is one of the best things that a mother can do to ensure a healthy start in life for their child. Smoking, Pregnancy and Fertility – ASH
Smoking in pregnancy increases the risk of pregnancy complications, such as stillbirth, preterm birth, miscarriage, low birthweight and sudden infant death syndrome (SIDS).
We know that pregnant mothers who live in areas of deprivation are more likely to smoke and that smoking increases the risks of pregnancy complications. Therefore, “those from lower socio-economic groups are at much greater risk of complications in pregnancy” LMS smoke free strategy
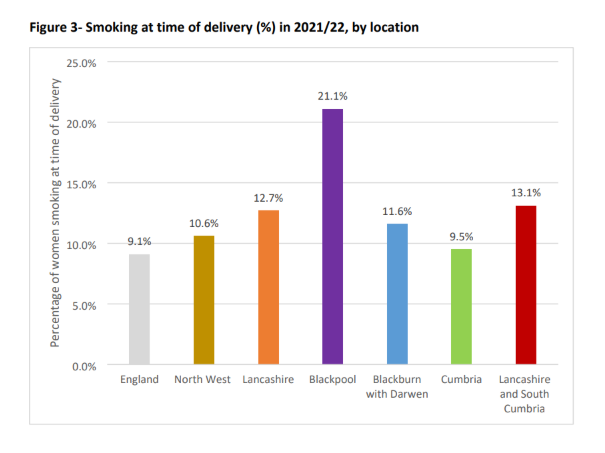
This graph is from the LMS Smokefree strategy. The stark reality of this graph is that in 2022 smoking at time of delivery rates in Blackpool were double the national average.
In addition to complications in pregnancy, further studies have shown that smoking during pregnancy has a far-reaching impact on the health of a child throughout their life.
Source: The NHS Long Term Plan
However, these studies have also shown that this can be reduced to that of a non-smoker if a successful quit is achieved early in pregnancy.
It is important to consider the effects of smoking on the whole life course and also it’s links to poverty.
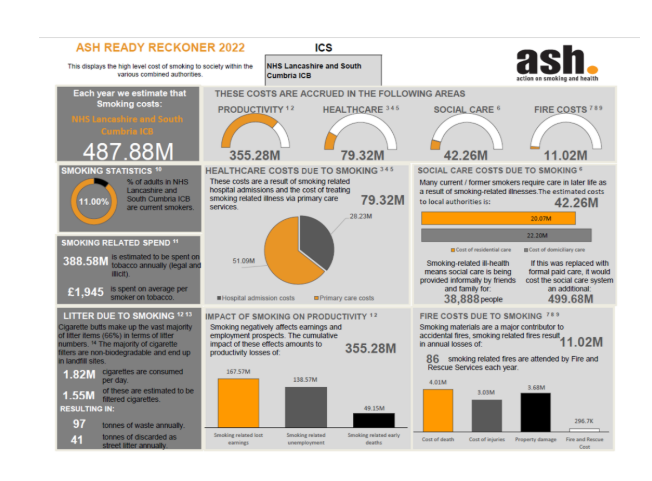
This infographic from Action on Smoking and Health (ASH) evidences the link between smoking and poverty.
Model Patient Pathway
NICE guidance on Smoking in Pregnancy recognises some pregnant people will find it difficult to say that they smoke as the pressure not to smoke in pregnancy is so intense; this in turn makes it difficult to ensure that they are offered appropriate support.
LSC are working towards the national pathway as a gold standard
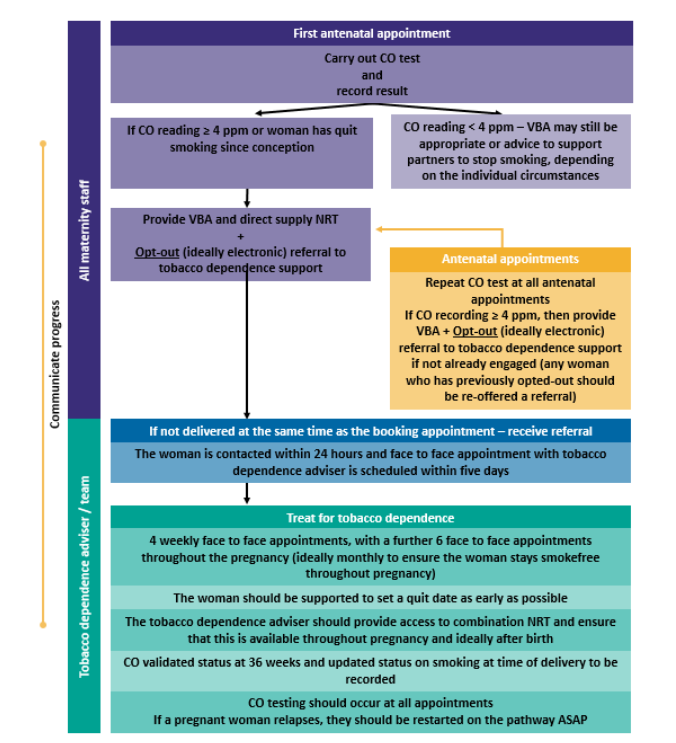
Development of the Smokefree Pregnancy Journey will support practitioners to follow the pathway for people who smoke during pregnancy.
Scenario: Pregnant or breastfeeding | Management | Smoking cessation | CKS | NICE
The plan (equity plan)
Each of the four trusts in the Lancashire and South Cumbria area employs a public health midwife and is now offering an evidence-based smoking cessation service with a financial incentive scheme in place in all trusts. NHS England » National smoke-free pregnancy incentive scheme
There has been a reduction in smoking at time of delivery Statistics on Women’s Smoking Status at Time of Delivery: England – NHS England Digital.
Public Health Midwives presented at the recent Lancashire and South Cumbria Smokefree Conference. Where there was a working group looking at supporting families better as they are having a high DNA rate at smoking cessation clinics. They are now trialling approaching this in a different way and have plans to introduce antenatal groups that will have smoking cessation at their core but not solely focused on this. This is alongside rolling out of the Continuity of Carer model which has had a positive effect on smoking rates in the areas where it is implemented.
Stop Smoking case study (youtube.com)

Smokefree Blackpool :: Blackpool Teaching Hospitals
Resources/Links
There are a number of external resources that can be used to support implementation and treatment of tobacco dependence:
- The NHS LTP website, providing background to our work on prevention (incl. tobacco dependence) https://www.longtermplan.nhs.uk/areas-of-work/prevention/treating-and-preventing-ill-health/
- Further resources from the National Centre for Smoking Cessation and Training https://www.ncsct.co.uk/ which also includes treatment programmes.
- Use of Local Tobacco Control Profile scan assist regional and ICS teams to have a clear map of local smoking behaviours and smoking related morbidity and mortality to inform implementation priorities.
- Resources developed by Action on Smoking and Health Smoking in Pregnancy Challenge Group http://smokefreeaction.org.uk/smokefree-nhs/smoking-in-pregnancy-challenge-group/
- PHE guidance on Screening and brief advice for alcohol and tobacco use https://www.gov.uk/government/publications/preventing-ill-health-commissioning-for-quality-and-innovation
- e-Learning for Healthcare, Alcohol and Tobacco Brief Interventions programme https://www.e-lfh.org.uk/programmes/alcohol-and-tobacco-brief-interventions/
- e-Learning for Healthcare, Supporting a SmokeFreePregnancy https://portal.e-lfh.org.uk/Catalogue/Index?HierarchyId=0_41043&programmeId=41043
- E-Learning for Healthcare, Making Every Contact Count https://www.e-lfh.org.uk/programmes/making-every-contact-count/
- PHE, All our Health: https://portal.e-lfh.org.uk/Component/Details/596376
- British Thoracic Society –Smoking Cessation Quality Improvement toolkit https://www.brit-thoracic.org.uk/quality-improvement/clinical-resources/smoking-cessation/smoking-cessation-qi-tool/
- Maternity and Neonatal Safety Improvement Programme: https://www.england.nhs.uk/mat-transformation/maternal-and-neonatal-safety-collaborative/
Equity and Equality guidance 4c Action on perinatal mortality and morbidity. Intervention 3: implement an LMS breastfeeding strategy and continuously improve breastfeeding rates for women living in the most deprived areas.
The NHS Long Term Plan (2019) stipulated that all maternity services that do not deliver an accredited, evidence-based infant feeding programme, such as the UNICEF Baby Friendly Initiative (Learn more about the UNICEF UK Baby Friendly Initiative), would begin the accreditation process in 2019/20. The new Fit for the Future 10-year health plan (2025) highlights in one of their case studies the inconsistencies that families can still experience when trying to access breastfeeding support:
“Care after birth was less good – we had issues with breastfeeding, and we received a lot of contradictory advice and felt a bit lost in the system.” Maryam, public participant, via the Change NHS website”.
Supporting optimal infant feeding practices remains a priority in Lancashire and South Cumbria.
Insights that inform the drive
Breastfeeding is the biological norm and deviations from this have health consequences, therefore promoting and protecting breastfeeding is a public health priority. Not breastfeeding increases the risks of illness and infections and has been linked to increased chances of obesity, maternal breast and ovarian cancer to name a few things (Off to the best start leaflet – Baby Friendly Initiative (unicef.org.uk)) .
“Reduced breastfeeding support, cuts in public health funding, negative attitude towards breastfeeding in public and a lack of knowledge of the health benefits of breast milk, all contribute to Britain having some of the worst breastfeeding rates in the world.” Why Britain has some of the lowest breastfeeding rates in the world | The Independent | The Independent
Infants born in the most deprived areas are least likely to breastfeed compounding health inequalities.
In the UK “lack of awareness and lack of consistent support” (Breastfeeding in the UK, Latest Stats and Rates from Experts. – Meet Anya.) have meant that breastfeeding rates are some of the lowest in the world with just 1% of infants being exclusively breastfed at 6 months.
This is compounded by marketing of commercial infant formula:
“The marketing of commercial milk formula for use in the first three years of life has negatively altered the infant and young child feeding ecosystem” Lancet 2023
Infant formula is marketed as a “the ‘normal’ or ‘ideal’ food for infants, rather than as a specialist product to be given if breastfeeding is not possible” (Conway et al 2023). This is despite the International Code of Marketing of Breastmilk Substitutes which was put in place to protect infants against marketing of infant formula being in place for over 40 years now.
Breastfeeding in the UK, Latest Stats and Rates from Experts. – Meet Anya.
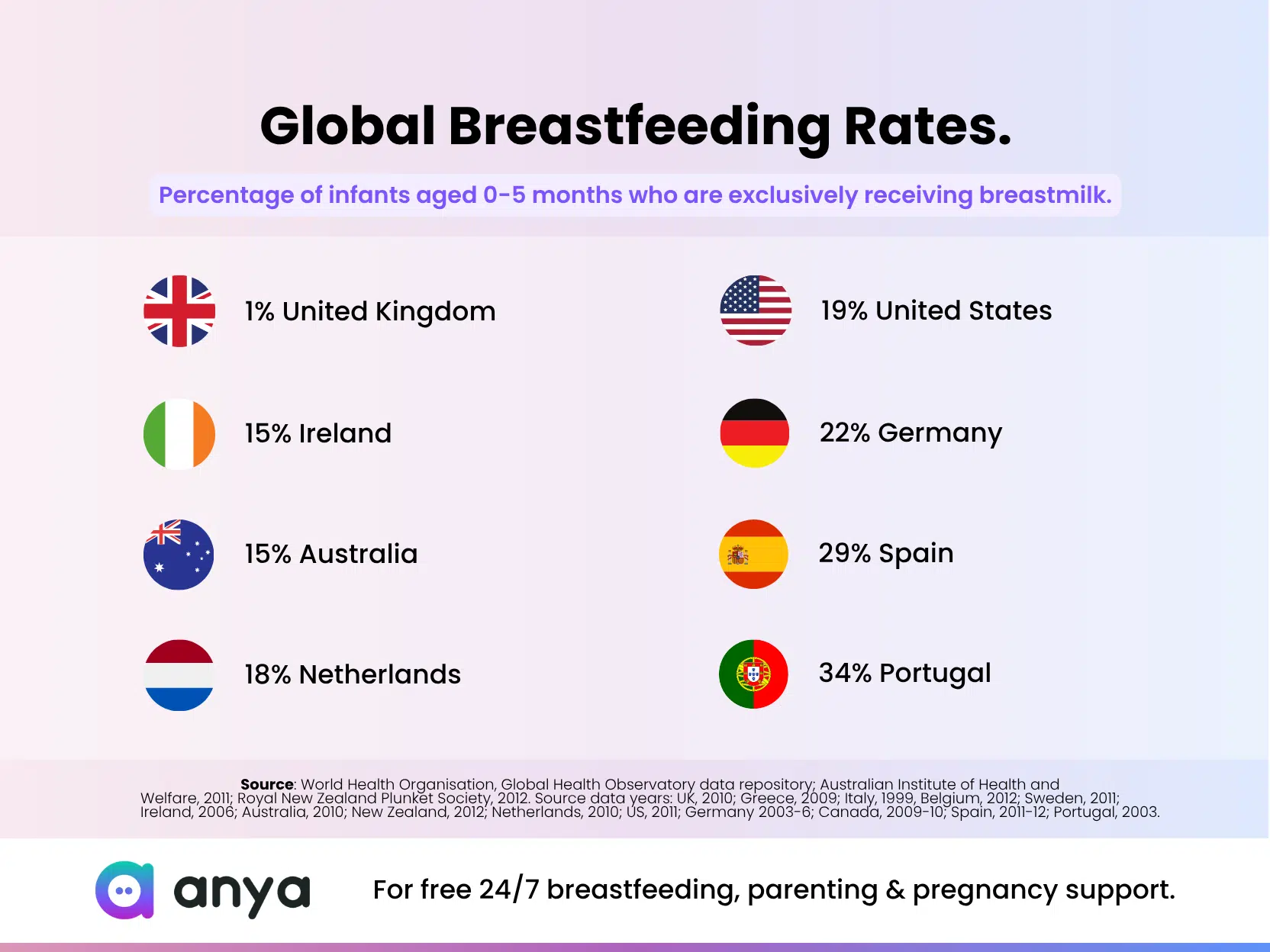
This infographic from Anya provides comparisons of exclusive breastfeeding rates across the world in the first 5 months of life with the UK being the lowest at just 1%.
{kind=link}
It is recognised that “women in who are most are disadvantaged are less likely to breastfeed” (NICE) thus compounding health inequalities and increasing poverty as the cost of formula increases (Unaffordable infant formula price rises: Safeguarding infant health and safety – Baby Friendly Initiative (unicef.org.uk)). There is substantial variation between parts of England, with over 80% of babies breastfed at 6-8 weeks in some parts of London compared with 32% in parts of the Northeast. To address health inequalities there must be improvement in breastfeeding rates for women living in the most deprived areas.
UNICEF highlight the fact that 8 out of 10 mothers cease breastfeeding before they wanted to. The approach needs to be systematic both addressing societal influences, addressing misconceptions and barriers through the wider communities but also improving care and support of mothers and infants.
Across Lancashire and South Cumbria all maternity and neonatal unit and community care services are working towards BFI accreditation.

This infographic from the World Health Organisation explains what is needed to support women to breastfeed; trained healthcare workers, paid time off work for breastfeeding and support for breastfeeding and returning to work, investment in breastfeeding support programmes, partners and families to support the breastfeeding mother, protection from formula marketing.
Fingertips 2023 report identified that across Lancashire the percentage of infants recieving breastmilk as their first feed is 33.5% which is below the national average Child Health Profiles (phe.org.uk) the wider variation of demographics across the Lancashire and South Cumbria patch means that there are some areas where breastfeeding rates are high compared to the national average.
Why is it important?
Evidence shows that breastfeeding has many benefits for young children, their mothers and therefore population health. Key findings from the Cost of Not Breastfeeding research paper were that 595,379 childhood deaths (6 to 59 months) from diarrhoea and pneumonia and approximately 974,956 cases of childhood obesity can be attributed to not breastfeeding according to global recommendations from the WHO and UNICEF each year. Also, approximately 98,243 deaths from breast and ovarian cancers and type II diabetes could be prevented each year by breastfeeding.
Infant health: Breastfeeding protects children from a vast range of illnesses, including infection, diabetes, asthma, heart disease and obesity, as well as cot death (Sudden Infant Death Syndrome)
Maternal health: Breastfeeding also protects mothers from breast and ovarian cancers and heart disease
Relationship-building: Breastfeeding supports the mother-baby relationship and the mental health of both baby and mother
Worldwide benefits: The benefits are seen in both high- and low-income countries, with a study published in The Lancet in 2016 finding that increasing breastfeeding rates around the world to near universal levels could prevent 823,000 annual deaths in children younger than five years and 20,000 annual maternal deaths from breast cancer
Cost savings:
Breastfeeding contributes to significant savings to the NHS, with initial investments paying off within just a few years. A NICE costing report estimates that Baby Friendly accreditation will start to save a facility money after three years, owing to a reduction in the incidence of certain childhood illnesses. Baby Friendly’s report Preventing disease and saving resources found that moderate increases in breastfeeding would translate into cost savings for the NHS of many millions of pounds, and tens of thousands of fewer hospital admissions and GP consultations.
A detailed “mapping tool” provided by Better Breastfeeding has been used to determine the gaps in the current service provision in each of the hospital trusts and local authorities in the LMNS. The vision set out in Better Births is quite broad. It states:
“The benefits of breastfeeding are clear. Breastfeeding improves children’s physical health by reducing infections, obesity, diabetes, allergic diseases, and sudden infant death; but it can also improve educational achievements and reduce social inequalities… [It] can provide the child with a natural safety net against the worst effects of poverty. The mother’s health will also benefit from reduced incidences of breast and ovarian cancers, diabetes, osteoporosis and coronary artery disease. Despite this, women told us that care was poor. There needs to be much better support for breastfeeding focused on practical help that supports and empowers women, rather than pressurises them.”
The Plan
There are several aims of the Infant Feeding project, which are to:
- ensure all staff understand their role and responsibilities in supporting expectant and new parents to feed and care for their baby in ways which support long term optimum health and wellbeing.
- enable all staff and supporters who have contact with new parents to provide full and competent support via appropriate training in infant feeding management and relationship building.
- encourage liaison / collaboration between health professionals, staff from other early years and children’s services, voluntary organisations and service-user forums, to deliver a seamless service and to develop a breastfeeding culture throughout the local community.
- set the standard for staff to adhere to, ensuring that families receive clear and evidence-based information, thus reducing the risk of families being given conflicting information about infant feeding.
- equip staff / supporters to support parents fully, ensuring that expectant parents are given evidence-based information to make decisions, and effective and timely support however they are feeding her baby.
- ensure high standards of professional practice, not to dictate the choices of parents.
- promote models of care that have a relationship building based approach for all families.
- create an environment where more women choose to breastfeed their babies, and where more families are given sufficient information and support to enable them to breastfeed exclusively for 6 months, and then for up to 2 years or longer in combination with solid food (for as long as mother and baby wish).
- The Infant Feeding Project supports the Baby Friendly Initiative (BFI) accreditation monitoring, including caregiver and staff audits and aims to ensure that the care provided improves outcomes for children and families, specifically to deliver:
- an increase in breastfeeding initiation rates
- an increase in the number of babies transferring home breastfeeding
- an increase in the number of babies discharged from the neonatal unit receiving breast milk
- an increase in the number of babies discharged from midwifery care breastfeeding
- an increase in breastfeeding rates at 10-14 days
- an increase in breastfeeding rates at 6 to 8 weeks
- amongst parents who are formula feeding, an increase in those doing so as safely as possible; fewer infants attending hospital with gastroenteritis
- improvements in parents’ experiences of care
- a reduction in re-admissions for feeding challenges under 28 days of age
- increases in the proportion of parents who receive information about the introduction of complementary food to their baby in line with nationally agreed guidance
We have already achieved…
An infant feeding network is now well established. This is comprised of infant feeding leads across the Lancashire and South Cumbria ICB from maternity, neonatal, health visiting and peer support services and now including a new paediatric infant lead at ELHT.
Roadmap for BFI accreditation:
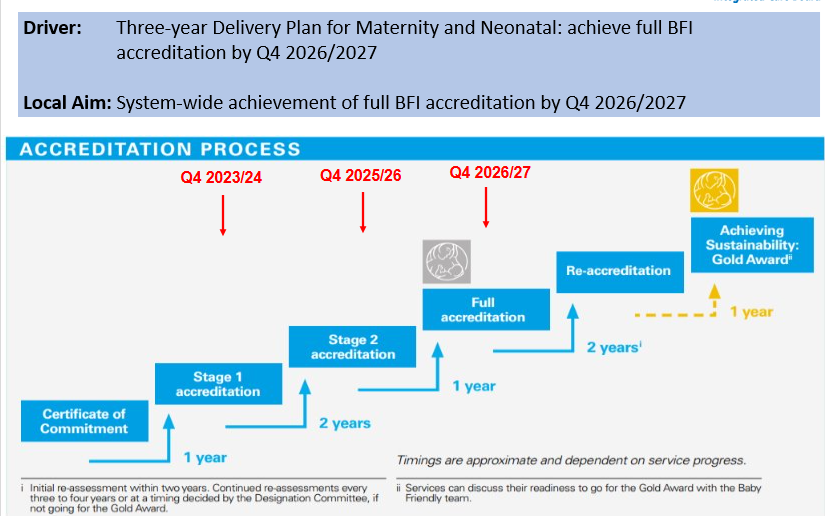
This slide shows the time frames that we need to meet to ensure that our providers are BFI accredited by 2027.
All acute NHS trusts have either achieved or are working towards BFI accreditation in maternity with one of our community providers and one of our acute trusts having already achieved BFI GOLD accreditation.
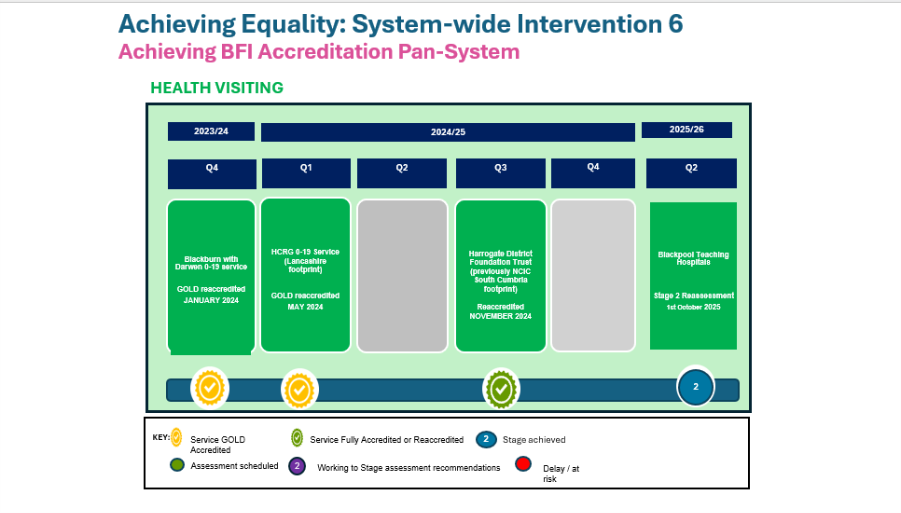
The slide above shows the community providers (who provide health visiting and school nursing services and Family Hubs/peer support). This slide shows that HCRG (who cover Lancashire) and Blackburn with Darwen services are GOLD accredited. Westmorland and Furness whose services have recently been taken over by Harrogate District Foundation Trust are fully accredited. Blackpool Teaching Hospitals community services are now stage 2 accredited and working towards stage 3.
Slide above shows BFI accreditation across maternity services. East Lancashire Hospitals Trust maternity services were GOLD re-accredited in June 2024. Lancashire Hospitals were stage 2 accredited in spring 2025. University Hospitals of Morecambe Bay were stage 2 accredited in September 2025 and Blackpool Teaching Hospitals have their stage 2 re-accreditation in November 2025.
Slide above shows the BFI accreditation status across neonatal services in Lancashire and South Cumbria. East Lancashire Teaching Hospitals are BFI accredited in their neonatal services, Blackpool Teaching Hospitals are stage 2 accredited and working towards stage 3. There is a working group at Lancashire Teaching Hospitals to put a business case in for a neonatal infant feeding lead as they currently do not have this. University Hospitals of Morecambe Bay neonatal unit have recently signed their certificate of commitment but do not currently have a specific infant feeding lead for neonatal.
The Lancashire and South Cumbria Infant feeding policy has been developed and is now in its 3rd iteration. Link to policy: LSC-IF-POLICY-AND-GUIDELINES-V3.4.docx
Positive feedback quotes on the infant feeding policy:
“It is comprehensive with underpinning evidence, (a lot of hard work and time has gone into this!) Haven’t got anything else to add. It also reads well!” HV Lancashire
“What an excellent document. Reads very clearly. I will do my best to deliver this information to my GP practice and look forward to trying to improve breastfeeding rates in my local patient population.” GP East Lancashire
“I’ve had read through and on the whole I think it’s really good, an interesting read and very detailed.” GP BwD
Developing the LMNS Infant Feeding Strategy
The Lancashire and South Cumbria LMNS Infant Feeding Strategy was developed through partnership working across maternity, neonatal, community and public health services. Health professionals, including midwives, health visitors and specialist infant feeding practitioners, contributed their experience to ensure the strategy reflects local needs and real‑life practice.
The strategy was shaped by listening to families’ experiences, helping to focus on personalised, compassionate support that respects individual circumstances, culture and beliefs. It is informed by national guidance and evidence and places a strong emphasis on equity, recognising that some families need extra support to access infant feeding services.
The strategy will continue to be reviewed and updated to ensure support for families improves over time.
Lancashire-and-South-Cumbria-Integrated-Care-Partnership-Breastfeeding-and-Infant-Feeding-Strategy.pdf
Leadership/ workforce
The infant feeding network comprises of infant feeding leads across maternity, community (including health visiting family hubs and peer support), neonatal, universities and now in East Lancashire paediatrics. This means that there is someone leading on BFI in all areas with ELHT being a pilot site for the new paediatric standards. These leads then have champions working with them who disseminate information and support staff. The network also reaches out to partner agencies for example social care and VCFSE organisations. It is pro-active so looks for ways in which to promote and protect breastfeeding in the communities which it serves.
In 2022 training was funded to increase the number of International Board-Certified Lactation Consultants (IBCLCs) across the Lancashire and South Cumbria footprint. This was to increase knowledge and expertise around breastfeeding in the workplace but to also to enable the provision on specialist care for complex infant feeding issues in all areas. This has been taken up by all trusts across the LMNS and some have gone further and continued to train further IBCLCs, supporting staff skills and knowledge across the teams. Specialist clinics have been set up in Lancashire where mothers and babies are able to access an appointment with an infant feeding specialist if they are finding that they are having complex issues that require additional support to that provided by the health visitor or local peer support. The plan is that each area will be able to provide this specialist service. IBCLCs and infant feeding leads who provide this care meet bi-monthly for clinical supervision and education and these professionals are supported to maintain their qualification by attending regular training and conferences.
This poster that was presented at the MAINN conference in 2025 explains the membership, achievements and future aspirations of the infant feeding network.
Infant feeding network members attending the 2025 MAINN conference.
Infant feeding network members holding the poster at the MAINN conference.
Training for staff
Start for Life unit has been working with NHSE to develop a new e-learning programme for the early years’ workforce. The programme aims to raise awareness of the links between breastfeeding and perinatal mental health, and the factors that can influence this relationship. It also provides tools and guidance to support staff to deliver self-reflective, person-centered care. It is aimed at anyone involved in providing support to families during the 1,001 critical days, including midwives, health visitors, infant feeding support workers, perinatal mental health specialists, psychological professionals and early years workers. It can be accessed on the NHS Learning Hub at the following link: Breastfeeding and Perinatal Mental Health programme.
BFI training for GP’s paediatricians and medical students E-Learning training packages – Baby Friendly Initiative (unicef.org.uk)
Resources
Better Births :: Infant Feeding Antenatal Information (icb.nhs.uk)
Better Births :: Preparing for birth and parenthood (icb.nhs.uk)
For families expecting babies soon, it has never been more important than it is right now to understand:
- Prolonged skin to skin contact, no matter how baby is born or fed, helps baby’s heart rate, temperature and breathing, gives better immunity and calms mum and baby.
- Every baby could benefit from their mother’s first milk, known as colostrum. This can be expressed and stored near the end of your pregnancy and given to baby.
- Babies who are breastfed have more protection from infection. All breastmilk is valuable, every drop counts.
For more information, ask your midwife, health visitor or breastfeeding support.
Information for those who are breastfeeding (opens in new window)
Information for those who are formula feeding their babies (opens in new window)
NICE guidance on faltering growth in children (opens in new window).
Care Pathways
Give an example of an infant feeding pathway for community and maternity.
Across Lancashire and South Cumbria, we are seeing increases in breastfeeding rates but there is still much work to be done.
A Parent’s Story: Specialist Infant Feeding Support
A mother was referred to the specialist infant feeding team after experiencing severe pain while breastfeeding. She had already been supported by her midwife and health visitor, but the pain made her feel unsure if she could continue.
At the time, the mother and her baby had recently moved in with grandparents after leaving an unsafe home situation. Breastfeeding was very important to her, for personal and cultural reasons, and she wanted to continue if possible. She was also feeling very upset and overwhelmed.
A specialist infant feeding practitioner offered an online appointment first, followed by a home visit to provide more hands‑on support. Care was tailored to the family’s situation, with a focus on both feeding and emotional wellbeing. With the right support, the mother’s pain improved and she felt more confident feeding her baby.
The mother and baby were then supported to attend a local family hub clinic, run by the same practitioner, as well as a friendly peer support group and midwifery clinic. Even after feeding challenges had been resolved, the mother continued to attend the support group and found it a valuable source of reassurance and connection.
With ongoing encouragement and personalised care, the mother went on to successfully breastfeed for over 18 months. When she later returned to work, she sent a message to thank the practitioner, saying she did not believe she would have been able to continue breastfeeding without the specialist infant feeding team’s support.
Case Study: Supporting Parents from the Trans Community
Every family’s journey into parenthood is different. This case study shows how respectful, inclusive care can make a real difference for parents from the trans community.
The Family’s Story
A trans dad (assigned female at birth) and his husband were preparing to welcome their second baby. During pregnancy, they spoke with their Mental Health Midwife about collecting colostrum (the first milk made before a baby is born).
From the beginning, the midwife took time to talk with the family about the words they preferred to use for their bodies, such as chest or breast. Agreeing this together helped the parents feel respected, understood, and comfortable discussing their care.
Planning Care Together
The family was referred to the Infant Feeding Team, who met with them to talk through their options. Together they discussed:
- collecting and storing colostrum before birth
- skin‑to‑skin contact after delivery
- feeding choices after the baby arrived
Plans were made for antenatal appointments, an elective caesarean birth, and postnatal support, with services working together to provide consistent and supportive care.
After the Baby Was Born
Although it had not been planned during pregnancy, after the birth the baby began receiving human milk from Dad. For up to nine weeks, the baby was fed expressed milk and, at times, fed directly from the chest.
With encouragement and support from staff, Dad felt safe and confident to respond to his baby’s needs. Feeling respected, correctly gendered, and supported by the healthcare team played a key role in their positive experience.
Why This Matters
This story highlights how small but meaningful actions—such as using the right language, listening without judgement, and offering flexible support—can make a big difference. Inclusive, person‑centred care helped this family to have a positive feeding experience and feel supported during an important time in their lives.
Every family deserves care that recognises who they are and supports them to make choices that feel right for them.
Breastmilk is magic – Be Well BWD
East Lancashire receives first maternity Gold Award – Baby Friendly Initiative East Lancashire Teaching Hospitals Trust maternity service was the first in the UK to achieve the GOLD BFI accreditation award.
Celebrating National Breastfeeding Week in Blackburn with Darwen – YouTube
ELHT NICU diary
Project Background and Progress:
The breast milk expressing diary was created to provide hands-on support for mothers as they express milk while their babies are in NICU. Recognising that mothers of preterm or poorly babies have unique needs, I wanted to create a resource that would be both informative and reassuring, helping them feel empowered and confident in providing breast milk. So far, the diary has been well-received, with positive engagement from both families and staff, who see it as an empowering tool that fosters connection and provides essential information.
Baby friendly guardians https://www.unicef.org.uk/babyfriendly/accreditation/achieving-sustainability/the-role-of-the-baby-friendly-guardian-infosheet/.
Junior Healthier Choices Award Blackpool Health Choice Awards
The Blackpool Healthier Choices award which is given to restaurants or takeaway establishments in the town and awards them according to having a hygiene rating of 3 or above and to be offering healthier options and for example using less salt and oil in the cooking process has now been extended to include a junior award.
This junior award recognises establishments that offers healthier choices and smaller portions for infants whilst also supporting breast and bottle feeding.
Across Lancashire and South Cumbria the importance of peer support in helping Mums and babies to achieve their infant feeding goals is recognised and there are two external providers used in Blackpool Henry- About us | HENRY and in Lancashire NCT NCT Infant Feeding Support Lancashire | About us | NCT, in Blackburn with Darwen peer support is provided in house from community providers. Westmorland and Furness also have plans to launch an in-house peer support service.
World Breastfeeding Week Celebrations at Blackpool Family Hubs
Photographs from Blackpool family hubs celebration for World Breastfeeding Week 2025.
In the future..
Local authority leads in the network alongside their NHS provider colleagues have now identified their priorities from the infant feeding strategy and are working towards these, alongside NHS providers. The strategy has numerous priorities and therefore it is not possible to work on them all at the same time. Therefore each local authority area in Lancashire and South Cumbria have identified their priorities. These have been prioritised with the needs of their communities in mind. Some examples of these are:
- Ensure that mothers feel comfortable to breastfeed throughout Lancashire and South Cumbria, and work to remove barriers to continued breastfeeding when they return to work
- Work with Early Years settings including Family Hubs and nurseries, and with schools to ensure that there are appropriate restrictions on the marketing on breastmilk substitutes, bottles, teats or dummies in schools and nurseries. Schools are informed about teaching resources on breastfeeding and encouraged to include this in their PHSE curricula
- Ensure that information about classes and appropriate written information on introducing solid foods (weaning) are well promoted and delivered in a setting and at a time which makes them accessible to the target population.
- Ensure that mothers who are least likely to breastfeed (as identified by the population health needs analysis) are identified antenatally and are provided with targeted support with feeding throughout their pregnancy and during their baby’s first two years of life. This may include families accessing the Healthy Start Scheme. Where targeted health visiting services are in place, these should be fully integrated with breastfeeding support services so that families receive additional and specialist support when needed.
- Families identified as being at high risk for child obesity are invited to take part in an evidence-based programme that has been shown to be effective in reducing rates of childhood obesity
- All Local Authorities should take part in a Breastfeeding Welcome scheme and publicise it with local businesses and families. The website or app in Action 18 may be utilised to share venues in the Breastfeeding Welcome scheme.
References/ further reading
Conway, R., Esser, S., Steptoe, A., Smith, A.D. and Llewellyn, C. (2023) Content analysis of on-package formula labelling in Great Britain: use of marketing messages on infant, follow-on, growing-up and specialist formula. Public Health Nutrition, 26(8), pp. 1696–1705. https://doi.org/10.1017/S1368980023000216
Rollins, N., Piwoz, E., Baker, P., Kingston, G., Matlwa Mabaso, K., McCoy, D., Ribeiro Neves, P.A., Pérez-Escamilla, R., Richter, L., Russ, K., Sen, G., Tomori, C., Victora, C.G., Zambrano, P. and Hastings, G. (2023) Marketing of commercial milk formula: a system to capture parents, communities, science, and policy. The Lancet, 401(10375), pp. 486–502. https://doi.org/10.1016/S0140-6736(22)01931-6
Genetic Risk Equity: Culturally-sensitive genetic services for close relative marriage.
Data, Service User Feedback or Patient Stories
Close relative marriage, sometimes known as consanguineous marriage, is the marriage of two people who are blood relatives. It is widely practised globally with 20% of the world’s population living in communities who favour consanguineous relationships, and 8.5% of births globally are to parents who are consanguineous.
The Born in Bradford study 2007-2011 found highest rates of close relative marriage amongst the Pakistani community – with 37% of Pakistani women married to their first cousin and a further 21% married to a more distant relative (Sheridan et al., 2013).
An autosomal recessive genetic condition occurs when both inherited copies of the same gene are faulty.
In the UK, this marriage pattern can be stigmatised, leading to fear of disclosure, mistrust of services and testing, a lack of knowledge and less opportunity to intervene at the earliest opportunity.
Why is it important (add tables etc) - for women, for fetuses / babies / long-term health of child, economy, education
Understanding the Relative Risk of Genetic Disorders
Recessive genetics conditions occur in all populations.
Children of related partners have a higher risk of inheriting two copies of the same faulty gene for a recessive genetic condition than children of unrelated partners. As a result, risk clusters in families.
The risk of still birth, infant death and disability is higher among communities practising close relative marriage – in the Asian Pakistani community, the risk of genetic disorders at birth for unrelated couples is 2.6% compared to a risk for related couples of 6.2% (Sheridan et al., 2013).
Congenital abnormalities cause 9.2% of stillbirths and 36.1% of neonatal deaths (MBBRACE-UK 2019p.153). They are the leading cause of infant deaths for Pakistani babies where the mortality rate from congenital abnormalities is 3.4 deaths per 1,000 live births. The rate for White babies is 0.74 deaths per1,000 live births (Li et al 2018).
Over 90% of babies born to cousin couples are healthy.
Slide as above. Narrative:
Service user insight alongside evidence from audit and published research identified;
Families often require support to share information with their family members
Persistent unmet need for information and support
Mixed experience of regional support reported. Sometimes families left the services lacking understanding and information about their choices
Extended families experience repeated, unexpected births of affected children and deaths. A significant number of which are attributed to recurrence in the same family
Families who do approach health practitioners for referral are sometimes refused
Lack in confidence to seek out services independently therefore families rely on health practitioner referral. More than 50% of families with likely auto-recessive disorder where not being referred.
The plan (Equity Plan)- what we have already achieved, what we are working on and what are our future plans- timescales
Lancashire and South Cumbria LMNS aims were:
Improve access to genomics services for underserved groups
Give families the opportunity to make informed reproductive decisions
Provide culturally competent genetic services
Co-production oversight group was established. Attendance of LMNS Lead, Public Health Lead, at National Communities of Practice this would include close relative marriage midwife and neonatal nurse and regional genomics associate once in post.
By achieving against these elements, there will be raised workforce awareness of referral/care pathways and optimised access to tertiary genomics services which will lead to:
- families receiving information at the earliest opportunity to inform their decision-making around their care options,
- a culturally sensitive, personalised care plan being developed by the woman and her family, with support from a skilled practitioner,
- if chosen, genomics screening being undertaken at the earliest opportunity,
- practitioners planning and preparing to meet the needs of the woman, infant and family,
- families planning for the care needs of the infant,
- families having improved experiences throughout pregnancy, intrapartum and postnatally,
- women and infants having improved health outcomes,
- the wider family understanding the implications for their own family planning and seek screening or diagnosis at the earliest opportunity.
Mapping aspirational touchpoints:
Workforce training delivered:
68 Midwives
6 Family Hub Champions
9 Health Visitor Champions
6 Local Authority PH Team
5 Home Start Practitioners
14 SEND Practitioners
22 Neonatal Staff
2 Paediatric Palliative Care Staff
Three strands change in national guidance 2024:
Training for Staff – how to book / access, how often to do, differentiated for role, mandatory update training.
Genetic Risk equity midwife and neonatal nurse provide in house training to ELHT staff.
Homestart East Lancashire provide training to the wider workforce.
Resources – patient information leaflets, links to more information, links to events (conversation starters link the maternity email address to access this resource)
Aide memoir for staff
Vaccination in Pregnancy
The three-year delivery plan for maternity and neonatal services that was published in March 2023 outlines the importance of evidence-based information and communication around vaccinations in pregnancy to ensure holistic care for women and the best start in life for babies.
The NHS Long Term Plan – 4c – Intervention 6: Vaccination against COVID-19 (seasonally), influenza (seasonally) and pertussis in pregnancy, including providing information in all contacts and across all settings antenatally, including where pregnant, women can get a walk-in vaccination; and working with regional vaccination leads to facilitate access to vaccination.
Insights
Vaccination in pregnancy programme and strategy was developed and leadership identified. A working group was formed, and this resulted in each of the four trusts in Lancashire and South Cumbria ICB footprint recruiting a public health midwife to lead on prevention programmes including vaccination.
Why is it important?
Immunisation programmes are essential public health initiatives designed to protect individuals and communities from infectious diseases. These programmes work by administering vaccines to people, which help their bodies develop immunity to specific diseases.
Vaccination during pregnancy is crucial for several reasons. Firstly, during pregnancy, a woman’s immune system is naturally weakened to protect the pregnancy, making her more susceptible to infections. Vaccines help protect both the mother and the baby from serious illnesses. Getting vaccinated against illnesses gives the newborn baby protection in the first weeks after delivery when they are at their most vulnerable to these illnesses and infections this alongside breastfeeding supports immunity.
Vaccines recommended in pregnancy
Flu
During pregnancy, your immune system (the body’s natural defence) is weakened to protect the pregnancy. This can mean you’re less able to fight off infections. As the baby grows, you may be unable to breathe as deeply, increasing the risk of infections such as pneumonia.
These changes can raise the risk from flu – pregnant women are more likely to get flu complications than women who are not pregnant and are more likely to be admitted to hospital. Having the flu vaccine means you’re less likely to get flu.
Having the flu vaccine during pregnancy also offers protection to the baby which means that they are less likely to develop flu in the early days and weeks of life.
The flu jab in pregnancy – NHS
Whooping cough (Pertussis)
Whooping cough is a very serious infection, and young babies are most at risk. Most babies with whooping cough will be admitted to hospital.
When you have the whooping cough vaccination in pregnancy, your body produces antibodies to protect against whooping cough. These antibodies pass to your baby giving them some protection until they’re able to have their whooping cough vaccination at 8 weeks old. The optimal time to have the Whooping Cough vaccine during pregnancy is after 16 weeks of pregnancy and before 32 weeks as this gives the best opportunity for the immune response and development of antibodies. However, you can have the vaccine right up until delivery and it will still provide some protection.
Whooping cough vaccination in pregnancy – NHS
Coronavirus (COVID-19) vaccine
If you’re pregnant, or think you might be, it’s strongly recommended you get vaccinated against COVID-19 to protect you and your baby.
You’re at higher risk of getting seriously ill from COVID-19 if you’re pregnant. If you get COVID-19 late in your pregnancy, your baby could also be at risk.
It’s safe to have the vaccine during any stage of pregnancy, from the first few weeks up to your expected due date. You do not need to delay vaccination until after you have given birth.
The COVID-19 vaccines do not contain any live viruses and cannot give you or your baby COVID-19.
Pregnancy, breastfeeding, fertility and COVID-19 vaccination – NHS
RSV
The RSV vaccine is now available for all pregnant women and should be offered around the time of the 28-week antenatal appointment.
RSV stands for respiratory syncytial virus and is the virus responsible for the development of bronchiolitis. Having this vaccination in pregnancy is the best way for a mother to protect her unborn baby from becoming ill with the virus as the mother develops an immune reaction boosting her antibodies which protect the baby from birth. In Lancashire and South Cumbria this is being made as easy as possible for expectant mothers to access with clinics being run in hospitals and communities and the vaccine also accessible in GP surgeries.
More information can be found at: RSV vaccine – NHS
BCG
The BCG vaccine is offered to babies that are in higher risk groups of developing tuberculosis. This may be because they live in a community where there has been an outbreak of the disease, or they or their family members have come from a part of the world where there is not an immunisation programme against tuberculosis, or of they live with a family who has or has had the disease. The TB vaccine is given at 28 days of age. The midwife or health visitor should refer for this.
BCG vaccine for tuberculosis (TB) – NHS
Chicken pox
Chickenpox (also called varicella) in pregnancy is uncommon because most adults in the UK are already immune, but it can be more serious if it occurs. If a pregnant person who is not immune catches chickenpox, it can cause complications for them and, in some cases, affect the baby, particularly if infection happens early in pregnancy or close to the time of birth. Anyone who is pregnant and has not had chickenpox before—or is unsure—and comes into contact with it should contact their GP or midwife urgently, as blood tests and treatments are available to reduce risks if given promptly.
Chickenpox and pregnancy | RCOG
The Plan
Leadership/ Workforce
Each of the four NHS trusts in Lancashire and South Cumbria now have a dedicated public health or health and wellbeing midwife who is responsible for leading the team delivering maternity vaccinations. Vaccinations are delivered in both hospital and community settings.
Training for Staff
We should work to the national PGD rather than the national protocol – which means that a registered health care professional should undertake all elements of the process from information giving to consent to drawing up the dose and checking, administration, documentation and immediate aftercare and advice. Please ensure that this has been approved by your organisation.
Resources
A guide on COVID-19 vaccine for women who are pregnant or breastfeeding (publishing.service.gov.uk)
Care Pathways
Comms
Comms to Service
i. It is important to have your vaccinations in pregnancy. Your seasonal Covid 19 and flu vaccinations are now due. Please speak to your midwife to find out how to book this, contact your GP or use the national booking system for COVID-19 vaccination via this link: Book, cancel or change a COVID-19 vaccination appointment – NHS (www.nhs.uk) and book your flu vaccination via your GP or using this national booking system link: Find a pharmacy that offers the NHS flu vaccine – NHS – NHS (www.nhs.uk)
ii. It is important to have your vaccinations in pregnancy. Now that you are 16weeks pregnant, your whooping cough (pertussis) vaccination is now due. Please speak to your midwife to find out how to book this or contact your GP.
Videos developed at LTHTr: https://vimeo.com/1020667451/b62a5db6ba – rsv
https://vimeo.com/938624865/cd6f16d7d8?share=copy – measles
Flu in Pregnancy https://vimeo.com/838610353/9325621773?share=copy
Whooping Cough https://vimeo.com/845276052/9e0618c8bd?share=copy
Pregnancy and Coronavirus (Covid 19) https://vimeo.com/855401258/90229c6ab3?share=copy
Leaflets on BadgerNet: https://www.gov.uk/government/publications/pregnancy-how-to-help-protect-you-and-your-baby and https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1043267/UKHSA-12222-COVID-19-vaccination-info-pregnancy-Dec21.pdf
Priority 4 of the Equity and Equality guidance calls for accelerated delivery of preventative programmes targeted at those at highest risk of poor health outcomes, with a specific sub‑priority on addressing perinatal mortality and morbidity. Lancashire and South Cumbria identified maternal nutrition as a key area of focus to support this aim.
Why is it important?
Ensuring optimal maternal nutrition during pregnancy is essential for the health of both the mother and the developing foetus, impacting short- and long-term health outcomes [1, 2, 3]. Poor maternal nutrition has been linked to adverse pregnancy outcomes, including low birth weight, preterm birth, and congenital anomalies. Adequate nutrition during pregnancy is also associated with reduced risk of maternal complications such as gestational diabetes and pre-eclampsia [1].
According to the latest National Health Service (NHS) statistics, in Lancashire and South Cumbria, nearly one in five pregnant women are classified as obese, increasing the risk of poor outcomes for both mother and baby [6]. Moreover, food poverty and insecurity remain major challenges, with many families struggling to afford healthy, nutritious food [7]. This can lead to an inadequate intake of essential nutrients and increase the risk of complications during pregnancy. Additionally, cultural beliefs and practices around food can also impact the dietary choices of pregnant women. These challenges are compounded by a lack of access to antenatal care and education, with some women not receiving any antenatal care until after their 12th week of pregnancy, which can lead to missed opportunities for interventions to improve maternal nutrition [8].
Women from minoritised ethnic communities and those who are most deprived face poor maternal and infant health outcomes [1-3]. The National Maternity and Perinatal Audit (NMPA) Sprint Report (2021) and wider literature [5], also report that women from South Asian and Black ethnic groups and those from the most deprived areas have higher rates of hypertension and diabetes compared to White ethnic groups and those from the least deprived areas.
Addressing these challenges requires a multi-faceted approach, including education and support for pregnant women, particularly those from disadvantaged backgrounds, as well as addressing food poverty and insecurity, and improving access to healthy foods and promoting healthy lifestyle choices. Health care professionals also need to be supported with information and education on how to have meaningful, personalised conversations and to make adequate referrals to appropriate, timely support.
Many health professionals in the United Kingdom feel ill-equipped to provide adequate nutritional advice to pregnant women. A survey of midwives found that only 47% felt confident in providing nutritional advice, with many citing a lack of training as a barrier to effective practice. Similarly, a survey of obstetricians found that only 27% felt adequately trained to provide nutritional advice to pregnant women [10]. These findings suggest that there is a need for increased training and support for health professionals to provide effective maternal nutrition care. Providing training and resources on topics such as healthy eating during pregnancy, managing gestational weight gain, and identifying nutrient deficiencies can help to ensure that health professionals have the knowledge and confidence necessary to provide high-quality care to pregnant women.
Despite the importance of optimal maternal nutrition during pregnancy, achieving it remains a challenge in many parts of the world. Key challenges to achieving optimal maternal nutrition include poverty, food insecurity, unhealthy dietary patterns, and lack of access to health care services. In high-income countries, unhealthy dietary patterns, such as excessive consumption of processed foods and sugar, can lead to maternal obesity and gestational diabetes, which can have adverse effects on both maternal and foetal health.
The Plan
To help work towards implementation of the action plan, UCLan and All4Maternity were commissioned to undertake a discreet package of work (Prioritising and addressing equality and equity needs in the Lancashire & South Cumbria LMNS footprint [PAN project]) that draws on quality improvement principles to help achieve clinical effectiveness and encouraging collaboration. This work was undertaken over three key stages to identify the problem (stage one), stakeholder engagement (stage two) and to identify solutions and resources to address the problem (stage three).
Maternal Nutrition has been identified, in stage one of the PAN project, as a key area to focus on to improve outcomes for childbearing women, people and families. This work will be informed by and undertaken alongside existing System-wide structures and activity.
Rapid evidence assessment on existing research was completed– focusing on successful maternal nutrition interventions with a focus on UK literature amongst populations with the greatest need – those from minoritized ethnic communities and living in lowest IMD deciles.
Dr Victoria Moran
Mapped existing local guidelines to national guidelines.
Collated existing national and local training, information and campaign resources
Mapped existing services, referral pathways and support available re: maternal nutrition
Debbie Gornall
Completed a training needs analysis for health professional staff and students (midwives, health visitors, students, GPs etc)
Dr Anna Byrom and Prof Gill Thomson
Completed consultation with service-providers, service-users as informed by reviews and scoping work
Debbie, Victoria, Anna, Lara
Developed of key resources/information/training materials as required
Timescales:
2023
January-March: Contracts, UCLan ethics (and R&D) approval. Stage one activities commenced.
April-June: Scoping reviews/mapping undertaken, consultations with healthcare professionals. Designing data collection tools and training community engagement advocates
July-August: Community engagement advocates collecting data from service-users. Staff training resources created.
September-Dec: Ongoing service-user and staff engagement
2024
January-March: Developed a framework of strategies and resources – final report writing
2025
Resources were shared with the midwifery and health visiting workforce
Resources
National Institutes of Health. (2010). Maternal nutrition and the outcomes of pregnancy. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3110651/
Centers for Disease Control and Prevention. (2020). Folic acid. Retrieved from https://www.cdc.gov/ncbddd/folicacid/about.html
World Health Organization. (2011). Iron deficiency anaemia: Assessment, prevention, and control. Retrieved from https://www.who.int/nutrition/publications/en/ida_assessment_prevention_control.pdf
Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. (2011). Dietary reference intakes for calcium and vitamin D. Washington (DC): National Academies Press (US).
NHS England. (2020). Maternity and neonatal health inequalities. Retrieved from https://www.england.nhs.uk/south-east/our-work/south-east-clinical-network/maternal-neonatal-health/health-inequalities/
Public Health England. (2018). Maternity care: women’s experiences. Retrieved from https://www.gov.uk/government/publications/maternity-services-annual-report/maternity-services-annual-report-2017-to-2018#antenatal-care
- Directive/ Drivers (why does this drive us (what we are being told to do by the ICB, National, NICE guidance etc))
The Innovation for Healthcare Inequalities Programme (InHIP) is a national NHS England initiative designed to tackle healthcare inequalities by improving access to proven innovations—such as medicines, diagnostics, and digital tools—for underserved and deprived communities. It is delivered in partnership with Integrated Care Systems (ICSs) and aligns with the Core20PLUS5 framework, which targets five clinical priority areas: maternity, mental health, respiratory disease, cancer diagnosis, and cardiovascular disease.
This infographic explains what core 20 plus 5 means. The core 20 being the most deprived 20% of the population and the plus groups being those that each ICS has chosen from their population. These are people who experience poorer than average health access. It then shows key clinical areas of health inequalities, these being; maternity, severe mental illness, chronic respiratory disease, early cancer diagnosis, hypertension and lipid optimal management and smoking cessation.
Insights (that inform the drive) – Data, Service User Feedback or Patient Stories
Pre-eclampsia is a serious pregnancy complication that typically develops after 20 weeks of gestation or shortly after childbirth. It is characterised by high blood pressure (hypertension) and protein in the urine (proteinuria), and can affect multiple organs including the liver, kidneys, lungs, and brain.
National Evidence
According to the latest MBRRACE-UK report and NHS data:
Black women in England are six times more likely to experience pre-eclampsia compared to white women.
Asian women are twice as likely to die during or up to six weeks after pregnancy compared to white women. [InHIP repo…r E&E page]
Black women accounted for 26% of cases where pre-eclampsia overlapped with chronic hypertension during childbirth, despite representing only 5% of all deliveries. [dearblackw…dgirls.org]
Studies show Black women are more likely to develop early-onset pre-eclampsia, which carries greater risks for both mother and baby. [bgmhfoundation.org]
These disparities are not solely explained by genetics or biology. Contributing factors include:
Higher prevalence of cardiovascular risk factors (e.g. hypertension, diabetes, obesity)
Socioeconomic inequalities (e.g. lower access to prenatal care, education, and nutrition)
Structural racism and healthcare bias
Nativity and acculturation: U.S.-born Black women have higher pre-eclampsia rates than foreign-born Black women. [hopkinsmedicine.org]
📍 Local Insights: Lancashire and South Cumbria
The InHIP maternity project and related initiatives have highlighted similar disparities:
Women from African, Caribbean, and Asian backgrounds in the region are at higher risk of severe adverse pregnancy outcomes, including pre-eclampsia. [InHIP repo…r E&E page]
The National Maternity and Perinatal Audit (NMPA) Sprint Report found that women from South Asian and Black ethnic groups have higher rates of hypertension and diabetes, which are key risk factors for pre-eclampsia. [maternity…ies report]
The E&E plan for MRH includes targeted interventions to reduce postpartum haemorrhage and improve clinical care for Black and ethnic minority women, acknowledging the link between pre-eclampsia and other maternal complications. [E&E plan f…H 29.01.25]
Access to Placental Growth Factor Screening insights
The focus of this part of the programme was to increase awareness and acceptability of the Placental Growth Factor Screening test, as one of the NICE accredited innovations for maternity.
During the duration of the project data from available laboratory tests performed show an increase use of PlGF screening testing:
Year
Tests performed at LTHTr
Tests performed at Blackpool
2022
259
14
2023
303
61
The project did identify a system-wide inequity of access to PlGF ratio testing, which is currently only offered at two of the four provider maternity units withing Lancashire and South Cumbria.
As such Phase two of the programme will look to address this inequity and seek to improve access to this NICE accredited innovation.
The data gathered as part of the 123 reported community engagement conversations and information sharing was able to demonstrate service-user and community acceptability of PlGF screening, as captured in the following data:
Have you previously heard of PlGF screening?
Only 13% of those who had data captured following engagement activity reported having knowledge of PlGF screening. This demonstrates the need to
For those that had heard of PlGF screening they rated their knowledge on average at a rate of 2.63 out of 5, indicating average knowledge.
Have you been offered PlGF screening in this or a previous pregnancy?
13 people had been offered PlGF screening out of 123. 22 were not sure or preferred not to say, or gave another response.
Of those who were offered the test, 9 had the test in their pregnancy and 3 did not have the test, a further 2 were unsure.
Of those that had the screening test, they rated their experience highly, with a rate of 4.44 out of 5:
When asked about their knowledge of PlGF screening following those who had data reported following their engagement gave their knowledge rating as 4.21 out of 5.
When asked if they would accept PlGF screening, following the engagement 93% (n=115 people) said yes, 6 said no and 2 were not sure.
This demonstrates how community engagement can enhance acceptability of screening programmes and health innovation mobilisation into practice.
Programme outputs
Series of digital training and engagement assets have been created to support optimal community engagement activity for maternity services: https://padlet.com/All4Maternity/inhip-maternity-programme-8o9kvfb080srhtim
Five core areas of impact
Increased community awareness and knowledge of pre-eclampsia including signs and symptoms and how to access care.
Evidence of service-user acceptability to PlGF screening
Developed staff/student/VS awareness and confidence of pre-eclampsia/ PlGF screening and community engagement approaches
Identifying system inequities – in relation to PlGF screening – not all maternity sites offering ratio assessment/analysis
Strengthening system working – including across multi-lateral and voluntary sector organisation, education organisations and health services. Engaged service-users in identifying preferences for ECoC service development.
Next steps for the programme into Phase Two based on the programme impact and learning so far.
Addressing inequalities of screening – some maternity units are not providing the full PlGF ratio screening – this can be reviewed at a system-level with Maternity Medical Directors
Strengthening Staff awareness of PlGF to increase use of the tool to inform care planning and informed choice for families.
Disseminating training to other family engagement settings e.g. Home Starts and Family Hubs across the system with the support of the existing community engagement leads.
Formalising student curriculum toolkit and student learning and engagement activity – working with engagement leads
Enhancing student engagement with the VOS and Charitable sectors exploring ongoing placement opportunities with Family Hubs and Home Start settings. This will help to strengthen collaborative working between these sectors and healthcare in the future.
Developing enhanced digital resources – including community engagement aid memoir resources and digital information resources for families, to be hosted on Badgernotes.
Encouraging the development of system-wide data lakes and reporting mechanisms that help to enable data dashboards for meaningful monitoring.
These next steps will be developed in collaboration with all key stakeholders and partners outlined in the section above.
- Priority 4c, (Local) Intervention 8:
CORALS Birth Afterthoughts Service
CORALS PROJECT
Co-develop and evaluate a new birth listening service for women who have unanswered questions / experienced a difficult or traumatic birth
What is a Birth Reflections service?
IT IS…..
Discussion with maternity professional/s
Opportunity for women/birth partners to tell story
Missing pieces and unanswered questions
Understand physiology of childbirth
Women and family led
Signposting/follow-up
IT IS NOT…..
Not counselling or therapy
Not a complaints service
Not a bereavement service
Evidence
Systematic review (Thomson 2024) – A rapid evidence review of postnatal listening services for women following a traumatic or negative childbirth experience – ScienceDirect (n=27)
Interviews with providers (n=24)
Interviews with service-users/consultations with marginalised populations (n=30)
Information gifted by West Yorkshire & South Tyneside and Sunderland MMH services
Co-produced (2.5 days) with:
Academics
Clinical lead/Clinical Psychologist
Specialist mental health midwives
Mental health practitioners
Service-user representative
Consultant midwife
ALL paperwork produced –
Care pathway
Screening script
SOP
Communication – email correspondence, information sheet, (translated 5
languages)
Templates – running and recording the session
Evaluation questions
Data recording form
Referral considerations presentation
Ethics approval for evaluation
Data sharing agreement with Trust
Piloted the training
Admin post…..resources to go live – Spring?
Pilot service over 6 months – evaluation – interviews, service-related data(referrals, reasons, number of meetings etc)
Project milestones and timeline
2023
January-March: Contracts, UCLan ethics (phase one).
April-June: Scoping reviews undertaken (phase one and two), consultations with healthcare professionals/service-users (phase one); consultations with healthcare professionals (phase two)
July-September: Co-production/ designing training and service user resources (phase one); training of community engagement advocates (phase two)
September-Dec: Finalising/developing resources for afterbirth debriefing services – training of nominated staff (phase one); Community engagement advocates collecting data from service-users (phase two)
2026
April: Evaluation of afterbirth/debriefing services (phase one); Develop a framework of strategies, actions and resources (phase two)
To be confirmed: Final report; dissemination activities
Lancashire and South Cumbria
Perinatal Pelvic Health Service
The NHS Long Term Plan (2019) committed to improve access to pelvic health physiotherapy and other specialists for all women and birthing people with pelvic health conditions during their pregnancy and after birth. Consequently, all women and birthing people across England should now have access to dedicated multi-disciplinary perinatal pelvic health services and pathways.
The Lancashire and South Cumbria (LSC) Perinatal Pelvic Health Service (PPHS) has been collaboratively developed across all sectors of care, to increase current service provision for those receiving maternity care at:
- Blackpool Teaching Hospitals NHS Foundation Trust
- East Lancashire Hospitals NHS Trust
- Lancashire Teaching Hospitals NHS Foundation Trust
- University Hospitals of Morecambe Bay NHS Foundation Trust
By increasing awareness, actively promoting a preventative approach, and enabling early identification of pelvic health symptoms, women and birthing people can access advice and treatment for pelvic health conditions during pregnancy and following birth. Ultimately, this should reduce the number of people living with pelvic health conditions postnatally and in later life, which can have a significant impact on bonding, attachment and overall quality of life.
Research shows that:
- 1 in 3 women and birthing people experience urinary incontinence in the first year after having a baby
- Up to three quarters of these women continue to experience this in the following 12 years after giving birth
- 1 in 10 women and birthing people experience anal incontinence (wind or stool)
- 1 in 12 women and birthing people will have a pelvic organ prolapse.
- Nearly 1 in 4 women and birthing people have never done pelvic floor muscle exercises.
Pelvic health issues are COMMON, NOT NORMAL following pregnancy and delivery, however is important that we normalise conversations about these problems. By reducing the stigma and appropriately signposting people to reputable resources and support in a timely manner, up to 70% of problems could be managed effectively.

Pelvic Health conditions include:
- Bladder and bowel problems
- Pelvic floor dysfunction
- Perineal trauma/Obstetric Anal Sphincter Injury (OASI)
- Pelvic organ prolapse
- Painful sex/pelvic pain
- Pregnancy-related musculoskeletal problems, such as:
– Separation of abdominal muscles (diastasis rectus abdominis)
– Pelvic girdle pain
– Back pain
– Carpal tunnel syndrome
Resources and self-referral
Each provider has its own webpage that provides support and resources on perinatal pelvic health.
In the first instance, women and birthing people are encouraged to use this information to prevent and self-manage any symptoms that may develop due to pregnancy and/or delivery. If, however, they remain symptomatic despite following the advice, self-referral is available at all trusts.
Resources and self-referral guidance for your local service can be accessed via the links below:
PPHS clinics
Each provider has a multi-professional PPHS clinic where women and birthing people are seen by midwives and physios in the same appointment, with direct or indirect oversight from a consultant obstetrician.
These clinics predominantly offer support to those who recently sustained an OASI during childbirth or have postnatal perineal/pelvic floor concerns, however they also provide opportunities to discuss birthing options for those who have had a previous OASI and are pregnant again.
Where indicated, women and birthing people are referred to specialist midwifery or physiotherapy clinics for ongoing advice and support.
Learning and development
The PPHS is committed to the education of the current and future workforce, to improve outcomes for women and birthing people across LSC.
Our PPHS midwives deliver OASI and Antenatal Preventative Pelvic floor Exercises and Localisation (APPEAL) training within their respective providers. This ensures that all clinicians supporting women and birthing people throughout the maternity pathway are aware of the current evidence base and its application in practice.
Working alongside our HEI partners, the team are now providing expert insight through guest lecturer opportunities on both midwifery and physiotherapy programmes. Where feasible, services support clinical placements, either as standalone or spoke offers, to link academic learning to the realities of practice.
Leadership placements and work-based projects support the PPHS’s strategic development, with specific focus on innovations to address health inequalities and KPI achievement.
Future work
The PPHS will continuously develop and improve in line with the three key shifts identified in Fit for the future: 10-year health plan for England (Department of Health and Social Care, 2025).
Planned activities include:
- Postnatal pelvic health self-assessment – phased rollout and implementation in collaboration with primary care partners, to support pelvic health discussion as per the GP 6-8 week maternal postnatal consultation – what good looks like guidance.
- Health inequalities – targeted projects to explore the PPHS’s inclusivity in relation to sexual orientation/gender identification, neurodiversity and age.
- Prevention – introduction of a system-wide approach to prevent pelvic health symptoms in pregnancy and later life.
| Reducing Racial Inequalities in Maternal and Neonatal Care |
| MBrace MBRRACE-UK: Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK | MBRRACE-UK | NPEU highlights the fact that women from black and ethnic minorities experience persistent inequalities in maternity care meaning that black women are 3 times more likely and Asian women 2 times more likely to die than white women during the perinatal and postnatal period. It identifies systemic racism. There are calls for a Safe Maternity Care Act to be put in place SAFE Maternity Care Act – Birthrights . Birthrights highlight the fact that “The voices of the most marginalised women and birthing people need to be centred throughout training, guidelines, policy, practice and legislation.” |
| Insights Lancashire Teaching Hospitals as part of their Race Health Observatory quality improvement project identified through baseline data that there was health inequality between population groups in relation to major obstetric haemorrhage. They identified that 12% of people from black and ethnic minority groups experienced postpartum haemorrhage over 1000 mls per week compared to 5% of white people. They aimed to reduce this from 12% to 6% by March 2025. |
| Clinical Impacts of PPH PPH is defined as blood loss exceeding 500 mL after vaginal delivery or 1,000 mL after caesarean section, and it can occur within 24 hours (primary PPH) or up to 12 weeks postpartum (secondary PPH). [my.clevela…clinic.org], [www.merckmanuals.com], [www.who.int] 1. Maternal Morbidity and Mortality PPH is the leading cause of maternal death worldwide, responsible for approximately 70,000 deaths annually. [www.who.int] Severe cases can lead to hypovolemic shock, organ failure, and death if not treated promptly. [my.clevela…clinic.org] 2. Physical Health Consequences Women may experience anaemia, fatigue, and delayed recovery. Surgical interventions such as hysterectomy may be required in extreme cases. Risk of reproductive disability due to uterine damage or complications from transfusions. [www.who.int] 3. Psychological and Emotional Trauma PPH can be a traumatic experience, leading to anxiety, depression, or PTSD. Women often report feeling unprepared or unsupported during emergency interventions. [my.clevela…clinic.org] Systemic and Service-Level Impacts 1. Clinical Governance and Review At Blackpool Teaching Hospitals, all PPH cases >2,000 mL are subject to rapid review and governance oversight. [05 PPH The…Oct 25 EM] Reviews assess parity, gestation, delivery mode, labour conditions, and staff presence to identify systemic patterns. 2. Health Inequalities Internal data from E&E plan for MRH 29.01.25 shows that Black and ethnic minority women are disproportionately affected: 12% experienced PPH ≥1,000 mL weekly compared to 5% of white women. Targeted interventions aim to reduce this to 6% by March 2025. [E&E plan f…H 29.01.25] 3. Clinical Practice Improvements Use of PPH risk assessment tools enables personalised care planning. Emphasis on real-time blood loss estimation and education for staff to shift from reactive to preventive care. [E&E plan f…H 29.01.25] Risk Factors and Prevention Key Risk Factors Uterine atony, retained placenta, genital tract trauma, bleeding disorders, and prolonged labour. [www.merckmanuals.com] Low body weight and pre-existing conditions (e.g. clotting disorders) increase vulnerability. [All Wales…(2.8)_2021] Prevention Strategies: WHO recommends uterotonics (e.g. oxytocin, tranexamic acid) and uterine balloon tamponade for prevention and treatment. [www.who.int] Early detection and bundled treatment approaches (e.g. E-MOTIVE trial) have shown cost-effective improvements. [www.who.int] This driver diagram from Lancashire Teaching Hospitals supports the aim to reduce PPH for black and ethnic minority people by 50%. This chart shows the local drivers identified. |
| The plan (Equity Plan) This quality improvement project decreased the incidents of PPH in the target population group from 12% to 9% This was achieved through staff education and resources. Challenging misconceptions and creating an awareness of the health inequalities within PPH experience. The emphasis was moved from managing PPH to prevention of PPH. This improved clinical care delivery and real time accuracy of blood loss estimation. The PPH risk assessment tool supported personalised care planning throughout pregnancy and labour and was adapted to reflect changes in individual circumstances. This piece of work was completed with the support and guidance of the NHS Race and Health Observatory. For service users this has meant improved accessibility to information through translation and digital innovation. Service user feedback: “I am glad to hear of the positive improvements being made” “I am personally grateful for the work you are doing and hope that many in the future will benefit”. |
| Future plans Continue to use anti-racism principles to affect positive change. Continue to create a safe environment for discussion and honest conversations. Sustain improvements through embedding relevant tests of change. Identify future opportunities including innovative communication solutions. This project has been presented and learning shared with the wider local maternity and neonatal system. |